A short summary of the nomenclature change
Whilst I have changed my primary research focus from metabolic liver disease to cholestatic/biliary fibrosis, I remain closely involved with the metabolic liver disease community, particularly as chair of the Steatotic Liver Disease Specialist Interest Group of ESPGHAN (SLD SIG). This is the new name for fatty liver disease. NAFLD is now ‘MASLD’ (metabolic dysfunction-associated steatotic liver disease). Here I am sharing some thoughts on the change in nomenclature.
The change from NAFLD to MASLD has happened for several reasons: it was a stigmatising term (both the reference to alcohol and the use of ‘fatty’) and it made it a diagnosis of exclusion. I.e. you only made the diagnosis of NAFLD if you ruled everything else out. The problem with that is: that it is quite common for individuals to have more than one liver diagnosis (e.g. autoimmune and steatotic liver disease). Also ‘non-alcoholic’ doesn’t really make sense for paediatrics because (significant, chronic) liver damage secondary to alcohol use is rare in children.
So an international group set about trying to establish a new name for NAFLD, and settled on MASLD. You can read the full paper in several places.
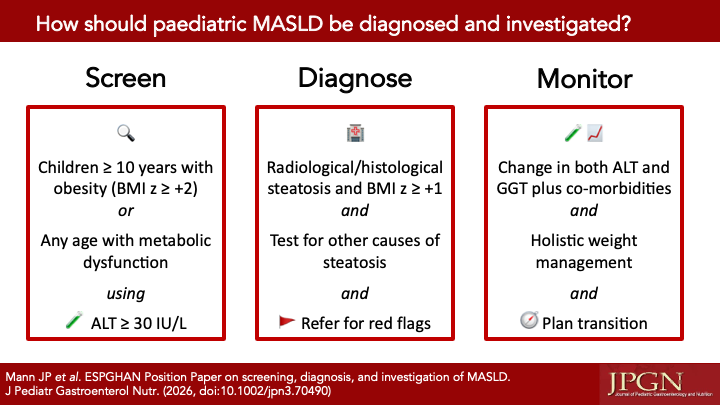
It now means that a diagnosis of MASLD can be made if individuals meet certain criteria plus have evidence of steatosis. This is essentially looking for surrogates of insulin resistance (‘pre-diabetes’) plus steatosis (fat infiltration of the liver cells. One challenge of this in paediatrics is that there isn’t really well accepted cut offs for those markers of pre-diabetes.
Prior to MASLD, some people were using the term MAFLD for a while (which I did also support). Coining this term helped pave the way for the use of MASLD. It had the positive step of criteria to ‘confer’ a diagnosis (rather NAFLD as one of exclusion), though still included the stigmatising term ‘fatty’.
Also, in paediatrics in particular, the “exclusion of other causes” part of diagnosing NAFLDi is really really important. That’s because we do see rare, genetic causes of steatosis more often than our adult colleagues do (e.g. Wilson’s disease). Missing one case would be devastating. So, despite moving to a model of conferring a diagnosing, rather than being one of exclusion, it is still important to test for the other causes of liver disease.
Another paediatric consideration is that we are more used to talking about ‘metabolic’ disease to mean ‘inherited metabolic disease’ (e.g. PKU, tyrosinaemia). This will take time to ensure clarity that when MASLD is discussed we don’t mean these kinds of genetic enzyme defects.
Overall, this is a huge step forward. It will encourage the use of positive language when we counsel patients. There will be challenges to its incorporation in the everyday use and we will need to work to move past them.
P.s. note that these are my personal thoughts only and do not represent those of my employer or any other society that I am a member of.